|
I have the opportunity, for which I’m so grateful, of not only attending this meeting but playing a role as a speaker, a sometimes stage “emcee,” and a keynote speaker. And as an attendee, I learn so much from other speakers, fellow attendees, and Medecision staff all sharing perspectives during breakouts and networking breaks. In mode of attendee (and self-confessed collegial-groupie of Dr. Topol’s), I took in his remarks taking notes as fast as I could thanks to Mom teaching me how to type on an IBM Selectric (the significance of which I wrote about here in the Huffington Post). Riffing on his great book, Deep Medicine: How AI Can Humanize Health Care, Eric started his talk donning my own professional hat as a heath economist, sharing data about America’s high health care spending with low ROI yield. “The U.S. is a distinct negative outlier,” the doctor noted, pointing to the detailed data from the OECD published in The Economist.
He showed new evidence from Nature (journal) Volume 574 dated 24th October 2019 — Eric is never guilty of showing old data unless it’s making a new-new insight. The article in Nature was “Quantum Supremacy Using a Programmable Superconducting Processor,” demonstrating that instead of 10,000 years to analyze data, the new analytics capability enables a calculation in a matter of seconds. Then Eric quoted Thomas Friedman’s January 2019 op-ed from the New York Times, titled, “Warning: everything is going deep.” Friedman, author of one of my go-to tomes, The World is Flat, called out that in 2019, “The word for the year is ‘deep,'” as in “deep learning, deep insights, deep artificial minds.” For Dr. T, it’s all about “Deep Medicine.” What can going deep in medicine do for health systems, health care, doctors and patients?
Here, he described the evidence demonstrating that statins work in only 18 of 1,000 patients, but of course statins are prescribed the world over in millions of patients, making the drug category one of the top prescription medicines on the Planet. This is the illusion of treatment that doesn’t do anything.” Instead, we need to do polygenic risk scores instead of taking statins, Eric argued based on the evidence for doing so published in JAMA and New England Journal of Medicine. “Polygenic risk scores are going to be the future.” So why aren’t these risk scores used by cardiologists, internists and PCPs today? Because of “sclerosis of the medical community,” Eric called it.
Finally — my most re-tweeted tweet during the session — Dr. T asserted that, “There is no room for hospitals in the future. It’s all about the patient’s bedroom.” Eric’s point wasn’t that we don’t need emergency and trauma services, ICUs and other brick-and-mortar health care sites for people who need care in complex settings. But for so many conditions that can be managed remotely and via self-care technologies enabled by broadband connectivity…we’re getting there. I quite concur: this is the last section of my book, HealthConsuming: From Health Consumers to Health Citizens. That paragraph imagines how our homes can and should be our health hubs, enabled by connectivity (ensuring net neutrality and fast lines for all), privacy and data security, and universal health care access. That, too, was a prime Dr. Topol moment, wearing his health policy hat: his belief that the U.S. as a “negative outlier” in the developed world is that way because the nation does not guarantee universal health care as a civil and human right. It’s not only AI that can help humanize health care. It’s people like Dr. Eric Topol living out bold thinking and bold doing. The post Learning from Dr. Eric Topol, Live from Medecision Liberation 2019 appeared first on HealthPopuli.com. Learning from Dr. Eric Topol, Live from Medecision Liberation 2019 posted first on http://drugsscreeningpage.blogspot.com/ via Blogger Learning from Dr. Eric Topol, Live from Medecision Liberation 2019
0 Comments
The 7th Annual U.S. Healthcare Consumer Survey from TransAmerica‘s Center for Health Studies underscores that Americans are “settling in” during a phase of “healthcare uncertainty.” The first chart illustrates the top sources of stress gauged in each of the past four years of this survey since 2016. Note that in 2019, many issues have spiked upward: healthcare costs, family, work, health problems affecting one’s family, personal health concerns, job stability, relationships, and personal safety.
TransAmerica found that people can’t typically afford health insurance premiums above $300 a month — that is, $3,600 for an annual premium for a health plan. Cost concerns create barriers for some people who don’t visit doctors or fill/take prescription drugs: 27% of Americans cancelled a medical appointment due to expected health care costs, and 22% said they did not take their prescription meds in the past year because the cost of the drugs was too high, TransAmerica’s survey found.
As a result of cost and health care financial concerns, one-half of employed Americans feel job-locked due to health insurance coverage at the workplace. Three in ten people had to leave a job because the company didn’t offer health insurance benefits. One-quarter of people stayed at their current job because they needed to keep their health insurance. An historical sidebar — the uniquely American challenge and stress of job lock has been studied for years as an artifact of employer-sponsored insurance in the U.S. Here’s a study the GAO wrote back in 2011 detailing the need to overcome this labor mobility problem, which is alive and well (and not in a healthy sense) in 2019 based on the TransAmerica study.
Note that workers’ contribution for family coverage across all firms was $6,015 in 2019. Compare this $6,015 to the $3,600 affordability premium stress/pain-point found in the TransAmerica survey. That’s quite a large chasm between these two numbers, about $2,400.
Money, the economy, health care costs — these three stressors are bound up together in the American’s personal and household health economy. That was the theme that started the first Health Populi blog post in 2007. My favorite Tom’s Shell sign, pricing petrol at the pump that year as “Arm” for regular, “Leg” for plus, and “First Born” for premium gas still resonates with the health care cost and family themes of this post, twelve years later. The post Americans’ Top Sources of Stress are Money, Money, Money and Family appeared first on HealthPopuli.com. Americans’ Top Sources of Stress are Money, Money, Money and Family posted first on http://drugsscreeningpage.blogspot.com/ via Blogger Americans’ Top Sources of Stress are Money, Money, Money and Family A recent report by the National Pharmaceutical Council provides an overview of seven different value frameworks. Specifically, the overview includes value frameworks developed by:
The paper has a number of nice comparison tables, including the following. The study also finds that the value assessment tools are influential. In a 2019 survey of 534 payers, 76% of respondents had previously used an ICER report, 24% had used the NCCN Evidence Blocks, 7% had used the ASCO framework, and 5% had used ACC-AHA. Other value frameworks (i..e., DrugAbacus, PPVF) had <2% use and IVI was not included in the survey.
The report, however, notes limitations of many of these frameworks including: a lack of patient centeredness, lack of transparency (with the notable exception of IVI), focus on evidence largely from clinical trials, a focus narrowly on pharmaceuticals, and either confusing output or output that provides a false sense of precision. In short, while there has been much progress on the value assessment front in the US in recent years, there is much work left to be done. Current Value Assessment Landscape in the US posted first on http://drugsscreeningpage.blogspot.com/ via Blogger Current Value Assessment Landscape in the US Listening to Osler Listening to the Patient Liberating Health Care at Medecision Liberation 201910/21/2019
“Listen to your patient; he is telling you the diagnosis,” Dr. William Osler is quoted to have said around the turn of the 20th century. Dr. Osler had been a strong advocate for the physician-patient conversation to inform the doctor’s diagnostic acumen and improve patient outcomes. This year is the centennial of Dr. Osler’s passing, so it’s especially timely that I introduce this post with his legendary assertion in the context of kicking off the 2019 Medecision Liberation conference. This meeting convenes the company’s clients, partners, and staff to share best practices, spark insights and learnings, and enable networking between people attending the meeting. There’s a lot of artfulness baked into the agenda and flow of this event, I learned last year when I attended my first Liberation (2018). I was engaged for that meeting to do my brand of “trend-weaving” throughout the conference, as well as be a featured speaker on the theme of consumerism in health care.
Health Populi’s Hot Points: “Liberation” in health care has many meanings. The word can connote freedom for clinicians to practice to the top of their license, and in a practice environment where technology is invisible and empowers diagnosis and patient relationships. Liberation can mean patients accessing services where and when needed, without friction of bias, inequities, healthcare deserts and shortages, or payment barriers. Another liberation riff is freeing data to be liquid and move freely (and securely) through the health/care ecosystem, as in Todd Park’s energetic mantra, “Data Liberación!” Stay tuned for the many flavors of “liberation” by following the hashtag #MedLiberate this week, 22nd through 24th October, as we explore Dr. Topol’s lens on how AI can humanize health care, Dr. Chacko’s learnings on the power of human-centered design in health, Gary Mendell’s work on de-stigmatizing mental health, Dr. Ungerleider’s understanding of engaging with grace at the end-of life, Nick Adkins’ empathic embrace of the power of connection, and other humanistic health insights which follow in Dr. Osler’s learned footsteps. Do read more about Dr. Osler’s pioneering approach to patient-centered medicine through the eyes of Dr. Paul Rothman, CEO and Dean of the Johns Hopkins School of Medicine, which Dr. Osler founded. The post Listening to Osler Listening to the Patient – Liberating Health Care at Medecision Liberation 2019 appeared first on HealthPopuli.com. Listening to Osler Listening to the Patient – Liberating Health Care at Medecision Liberation 2019 posted first on http://drugsscreeningpage.blogspot.com/ via Blogger Listening to Osler Listening to the Patient – Liberating Health Care at Medecision Liberation 2019 In many cases, the answer is ‘no’. At least that is the findings from a paper by Ryan and Sood (2019). As reported in FiercePharma:
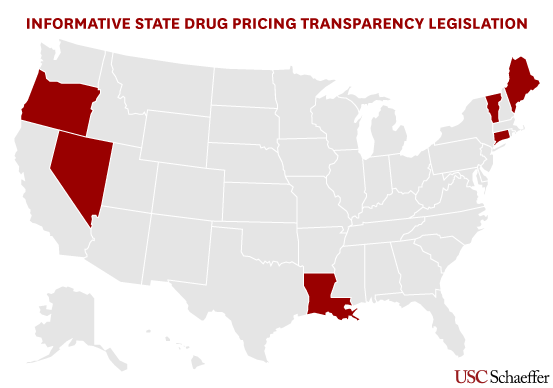
This study is especially informative as lawmakers have tried to require pharmaceutical manufacturers to disclose drug prices in advertisements, although this mandate has been struck down by the courts. Are drug price transparency laws informative? posted first on http://drugsscreeningpage.blogspot.com/ via Blogger Are drug price transparency laws informative?
Caregiving in the U.S., the seminal report from AARP, estimated that 43,5 million adults in the U.S. had provided unpaid care to an adult or child in the past year, about one in five people being caregivers. Over half of caregivers are women, and are about 49 years of age on average. Caregivers spent over 24 hours a week providing care go loved ones, and particularly time-intensive for spouses and partners. Most caregivers help a loved one with at least one Activity of Daily Living (ADL) which include eating, bathing, dressing, transferring (from bed to chair for example), maintaining continence, and toileting, which includes personal hygiene….like shaving. I’m frequently asked these days to address questions about social determinants and retail health for consumers’ self-care. The user-centered research, design, innovation, marketing and sales channeling of the Gillette TREO razor speaks to this convergence. Fast Company called the TREO “a masterpiece of inclusive design.” The Gillette TREO is the first product designed for, as P&G puts it, “assisted shaving.” Here’s a video that tells a story about the TREO. If you’re already a caregiver, this will resonate with you. If you’re not yet caring for a loved one in this way, just wait some months or a few years. Your time will come. Caregiving is the great equalizer as we benefit from cures and therapies that extend our lives…but can diminish physical and mental capacity if the dice roll that way. The image above for the TREO, “A Razor Designed for Caregivers,” is a scan of an ad I read in the October 2019 issue of the AARP Magazine featuring Tom Hanks on the cover (promoting his upcoming movie, A Beautiful Day in the Neighborhood, a biopic on Mr. (Fred) Rogers. On the page following this full-page ad was the “Upfront” interview with Julie Andrews who, after losing her voice following a vocal cord operation went wrong, has reinvented herself as an author of books working with her daughter — speaking of self-care and caregiving. Health Populi’s Hot Points: I had the (happily and tearful) pleasure of watching the video, below, at the recent GMDC SelfCare Summit where the Unilever team shared their commitment to and insights into the power of diversity — in this case, evolving and broadening concepts of “beauty.” This was done for the Dove brand, but is relevant in terms of reaching out to peoples’ inner lives and values beyond a product on a store shelf or medicine in a bottle. This is a great example of marketing in the New Retail Health era. Healthcare can and should learn about product innovation, education and marketing from across the health/care ecosystem in touch-points where patients, consumers and caregivers live every day lives seeking trust in relationships with organizations that bolster personal and family health. Increasingly, both consumer health and health/care companies will embrace this ethos if they intend to be relevant and resonant with health consumers – now, patients-as-payors. The post How a Razor Bolsters Health, Wellness and Love for Caregiving appeared first on HealthPopuli.com. How a Razor Bolsters Health, Wellness and Love for Caregiving posted first on http://drugsscreeningpage.blogspot.com/ via Blogger How a Razor Bolsters Health, Wellness and Love for Caregiving
Americans face high costs and hassle factors in health care. But more people are taking care into their own hands, and welcome a growing role for technology to play in enabling self-care, supporting prevention, and improving treatment of diagnosed conditions, according to The Future of Connected Health, a consumer survey from ResMed. For this research, ResMed interviewed 3,001 U.S. adults in June 2019, asking people to share perspectives on their health care experiences, the role of technology in healthcare, and devices they’d use to manage their care. Most Americans feel it should be easier to find the medical care that is best for them, and are sick of feeling like their personal health doesn’t matter in the current health care system. Four in ten consumers avoid going to a primary care visit because they’ve had bad experiences — that’s 1 in 4 Boomers and 6 in 10 Millennials.
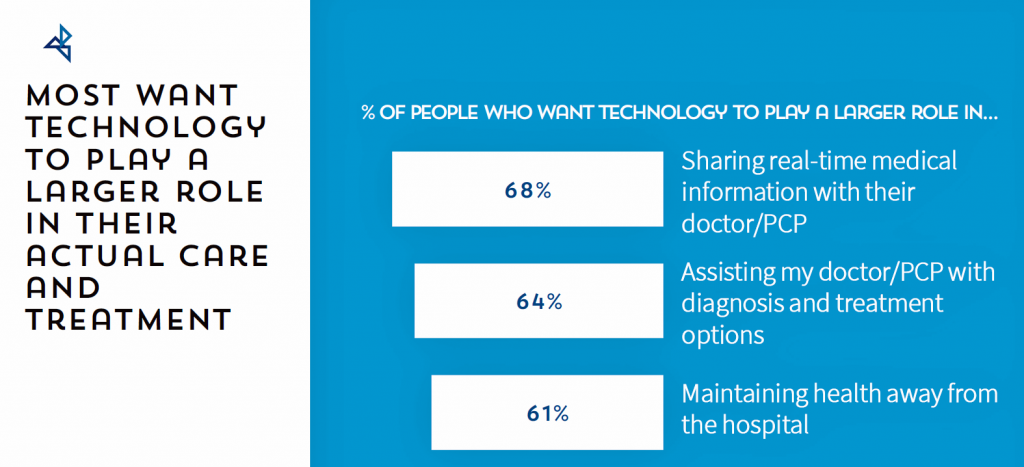
What’s the prescription to heal those frustrations? Technology. Six in ten consumers try to self-diagnose after browsing symptoms on the Internet including one-half of Boomers and three-quarters of Millennials. Again, six in ten people think they can identify the best treatments through their research without going to a hospital, true for one-half of Boomers and three-fourths of Millennials. These datapoints demonstrate that self-diagnosing online (aka “paging Dr. Google”) is a new normal — and not just for younger people, but for one-half of Boomers, as well. That underpins peoples’ perceptions where most agree that tech has made seeking medical treatments easier, and given people more peace of mind when dealing with their personal health issues, ResMed found. Most consumers want technology to play a greater role in addressing hassles and negative experiences in U.S. health care. A majority of Americans want tech to help them share real-time medical information with their clinicians, assist those clinicians with supporting diagnosis and treatment options, and bolster personal health outside of the hospital inpatient setting.
While most consumers in the ResMed study were bullish on the promise of technology to improve the quality and access of health care in America, people did identify drawbacks and barriers to achieving those outcomes. Over four in ten people thought digital technology makes getting medical care more difficult, not less, such as getting treatment for a medical condition and managing their personal health care. To get the most out of digital health technology, consumers need to better understand how those tools can help them self-care and more effectively connect with their clinicians and other care providers. There’s optimism for this, because over one-half of the ResMed study respondents said that technology has already improved their relationship with their doctors. That’s a trusted relationship already in place.
But patients don’t have as much patience to wait for the health care system, Big Pharma or politicians to make health care better. Patients – as consumers and voters – look to the technology industry to improve the quality of health care in America, the fourth chart illustrates from a RealClear Politics Poll conducted earlier this year. As Dr. Kvedar has demonstrated through his many years as a pioneer leading the Center for Connected Health, it’s the entire health/care ecosystem that must collaborate to make health care better with the Quadruple Aim in mind — to support patients’ outcomes, enhance the care experience, bolster clinicians’ energies to prevent burnout, and lower per capita costs. But as the centrality and primacy of the social determinants of health come into greater focus and importance in the mix of what makes health care, we can’t pin all our hopes on technology to Uber or Lyft us out of our fragmented and high-cost-by-design health care financing and delivery system. Public policies for agriculture and nutrition, transportation, labor, communications and education among them set the table for health. That’s where those “Dems in Congress” and “GOP in Congress” come into the mix, and a minority of Americans, soberly, see those folks as being part of improving the quality of health care in America. And trust — that’s the key currency here, underpinning all health engagement across the continuum of well-to-unwell people. As Neil Jordan, General Manager of Retail Health at Microsoft said in an on-stage interview at the conference, “You only get to blow trust once, you only get to get it wrong once…the relationship between the caregiver, provider and patient in this case is one of the most trusted elements out there…smart retailers are understanding that and using [it] in a positive way — working with providers in the community, to become part of that trust circle, using the brand to do that rather than actively competing.” That trust is in our barbershop, our church, our medical cannabis storefront, our retail pharmacy, our school, in our car, at a wellness retreat in the country, and especially in our home. Jordan’s taken a page out of my book, HealthConsuming, from “The New Retail Health” chapter, illustrated here. Health is everywhere, and our trusted touch-points for health are “ours” based on our own metric of value + values. Technology can help scale making health to where we live, work, play, pray, learn and shop. The post Most People Want Technology to Play a Bigger Role in Their Health Care, ResMed Finds appeared first on HealthPopuli.com. Most People Want Technology to Play a Bigger Role in Their Health Care, ResMed Finds posted first on http://drugsscreeningpage.blogspot.com/ via Blogger Most People Want Technology to Play a Bigger Role in Their Health Care, ResMed Finds
For years, Alegeus found that patients were indeed growing those consumer health muscles to save and shop for health care. In 2019, it appears that patients have backslid, according to the 2019 Healthcare Consumerism Index from Alegeus. For this annual study, Alegeus surveyed 1,400 U.S. adults in September 2019 on issues concerning health care costs, shopping, value, saving and spending. The first chart shows that the 2019 Index fell from 60.1 points in 2018 to 57.9 in 2018. The Index is a sum of the consumer’s cost/value orientation and purchase behavior.
While two-thirds of consumers say they understand their insurance coverage, only one-half of them can correctly answer questions about the definition of premiums and deductibles.
What consumers are especially keen on is their price or personal cost of paying for health care. 70% of consumers were very focused on getting the best value-for-money spent on health care, 71% researched conditions and symptoms online, and 61% of people researched provider ratings. Even with that growing time spent on research, compared with studying other consumer good investments — like buying a TV or a car, choosing a mobile phone company, or booking travel — consumers spend much less time seeking information on health care services, shown in the third chart.
Still, healthcare savings lacks behind that for retirement, emergency funds, and college. The cold fiscal reality of healthcare costs in the family budget are that, once people reach retirement age, they’ll need close to $300,000 to cover out-of-pocket health care spending until they pass away. That’s in addition to what Americans had already saved into Medicare. Given that the average savings in a U.S. bank account was $8,863 according to this Bankrate study, we need to spread the words that, “It’s the Prices, Stupid” for American patients — now major payors of health care services. The reality is that patients really are big payors in American health care. Traditionally the U.S. health care industry has conceived of “payors” as employers, health insurance plan sponsors like government agencies, and unions. Add patients to that definition. And if Alegeus’s Index for 2019 is correct and people’s health consumer work-flows have eroded, we in the health/care ecosystem have a key mission to take on in 2019 and over the near-term: that is, to educate Americans to be their own best health economists for themselves and their families. And by the way, this is why my new mantra is that, “all health/care is retail.” The post Health Consumer Behaviors in the U.S. Stall, Alegeus Finds in the 2019 Index appeared first on HealthPopuli.com. Health Consumer Behaviors in the U.S. Stall, Alegeus Finds in the 2019 Index posted first on http://drugsscreeningpage.blogspot.com/ via Blogger Health Consumer Behaviors in the U.S. Stall, Alegeus Finds in the 2019 Index This is the question a paper by Chambers et al. (2019) aims to answer. The authors analyzed coverage decision of 204 drugs (or 409 unique drug–indication pairs based on information from the Tufts Medical Center Specialty Drug Evidence and Coverage (SPEC) database. This database contains coverage information for 17 or the top 20 health plans in the U.S. They authors use this database to evaluate whether the payers imposed restrictions such as:
Using this approach, the authors find that:
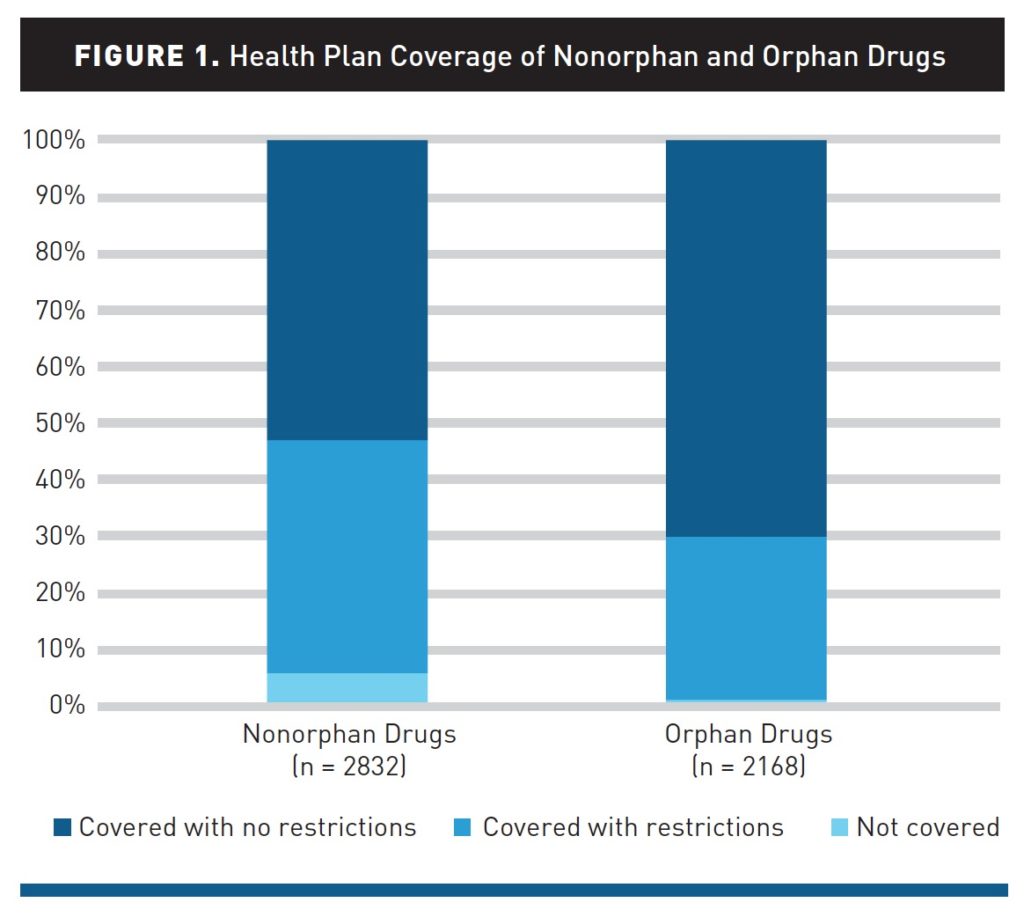
These average do hide some variability. The most generous plan covered all orphan drugs with only 11% having any restrictions, whereas for 2 of the 17 plans considered in the study, 50% or more of orphan drugs had some restrictions on access. How likely are U.S. health insurers to cover drugs for rare diseases? posted first on http://drugsscreeningpage.blogspot.com/ via Blogger How likely are U.S. health insurers to cover drugs for rare diseases? The U.S. has a gun problem. A paper by Goldstick et al. (2019) use data from the CDC’s Wide-ranging Online Data for Epidemiologic Research (WONDER) tool and find that:
Thus, clearly there is a problem with firearm-related mortality. Gun control activists would say the issue is that there are too many guns on the street. Those fighting for gun rights would argue that other factors are causing people to use guns to cause harm rather than to protect oneself. Regardless, these figures are clearly too high and we need an honest debate about what can be done to bring down gun-related homicides and suicides. Source:
Statistics you need to know: Firearm-related mortality posted first on http://drugsscreeningpage.blogspot.com/ via Blogger Statistics you need to know: Firearm-related mortality |
Anthony Williams
I am an experienced pharmacist with interest in content writing. I am also a known blogger for Drug Home Health Testing, an online drug testing and home health business. I write mostly about drug tests but many more from this sector will be coming soon. I am also a top selling author of Drug Test Dilemma! I have previously run a membership site for Drug home test making it in the most convenient way and the same knowledge has been compiled to create my new project Drug Test Dilemma. Personal Links |
 “Bold thinking is great. Bold doing is better,” Dr. Eric Topol introduced his talk yesterday at Medecision’s Liberation 2019 conference.
“Bold thinking is great. Bold doing is better,” Dr. Eric Topol introduced his talk yesterday at Medecision’s Liberation 2019 conference.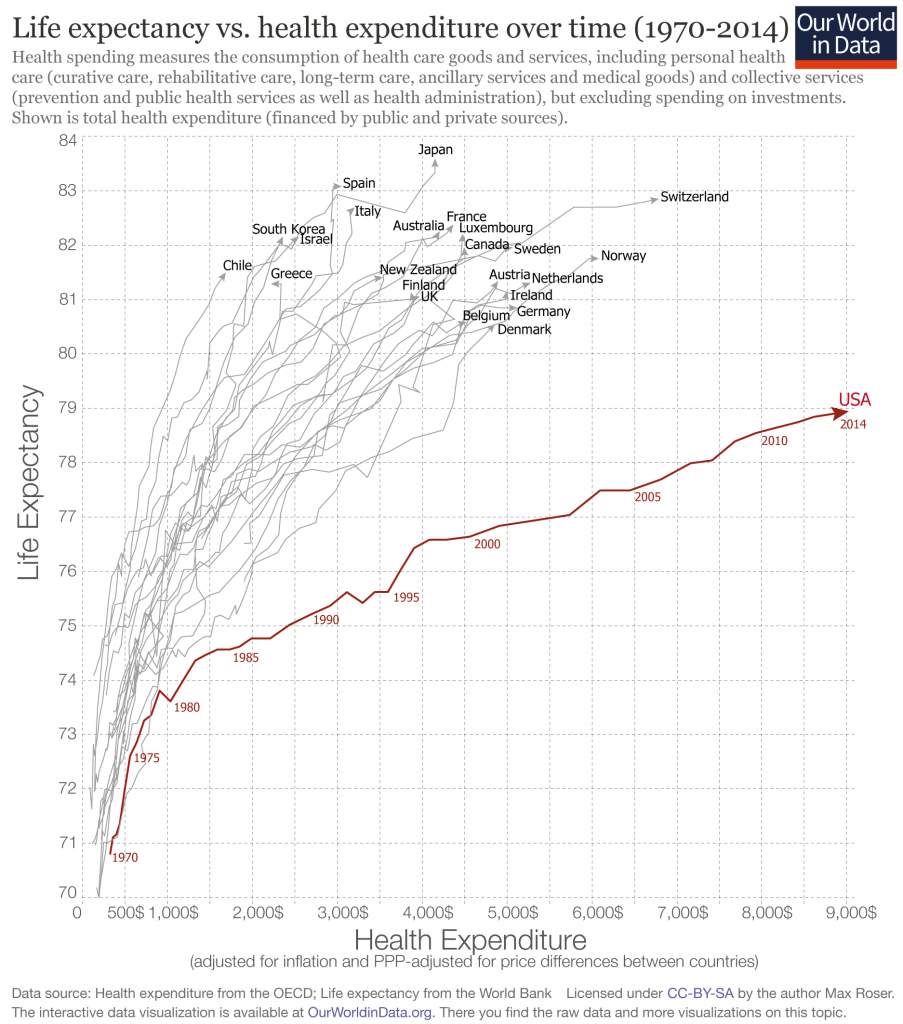 More people going into health care jobs, he continued, with the latest data from the Bureau of Labor Statistics illustrating that we’re adding more human capital to a broken health care system. “This isn’t the answer to our problem,” Eric asserted.
More people going into health care jobs, he continued, with the latest data from the Bureau of Labor Statistics illustrating that we’re adding more human capital to a broken health care system. “This isn’t the answer to our problem,” Eric asserted.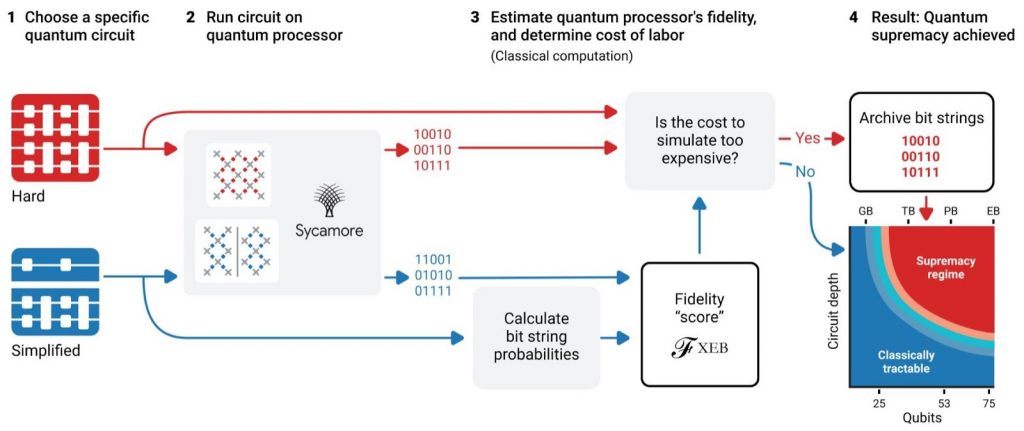 Eric offered several prescriptions, #1 being to use evidence to underpin workflows, diagnoses and prescribed therapies and procedures.
Eric offered several prescriptions, #1 being to use evidence to underpin workflows, diagnoses and prescribed therapies and procedures. He continued his prescriptions for making health care more human, humane, and evidence-based with other bold ideas including getting rid of keyboards in the physician-patient encounter, ensuring patients own/control their personal health data, and increasing the time shared between doctors and patients during the encounter.
He continued his prescriptions for making health care more human, humane, and evidence-based with other bold ideas including getting rid of keyboards in the physician-patient encounter, ensuring patients own/control their personal health data, and increasing the time shared between doctors and patients during the encounter.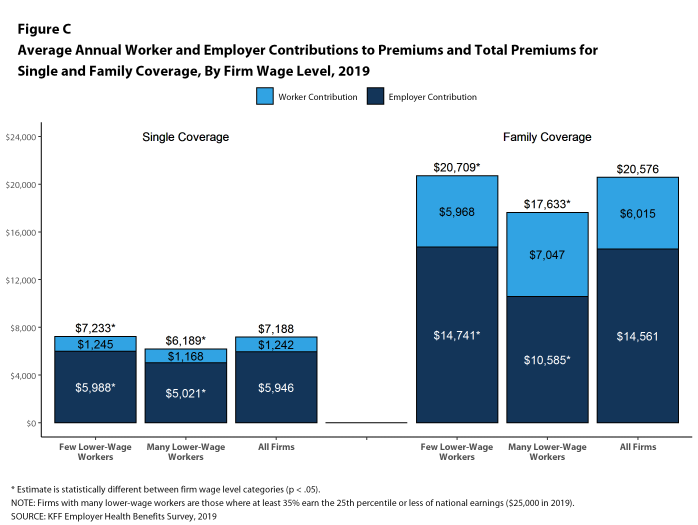 This latter point was emphasized in the survey noting that 71% of Americans said that drug prices were too high; 78% of people agreed that the government should be permitted to negotiate/regulate prescription drug prices.
This latter point was emphasized in the survey noting that 71% of Americans said that drug prices were too high; 78% of people agreed that the government should be permitted to negotiate/regulate prescription drug prices. That affordability data point is shown in this last line chart from the TransAmerica survey, illustrating that $300 is the total affordability median amount for a monthly premium payment.
That affordability data point is shown in this last line chart from the TransAmerica survey, illustrating that $300 is the total affordability median amount for a monthly premium payment.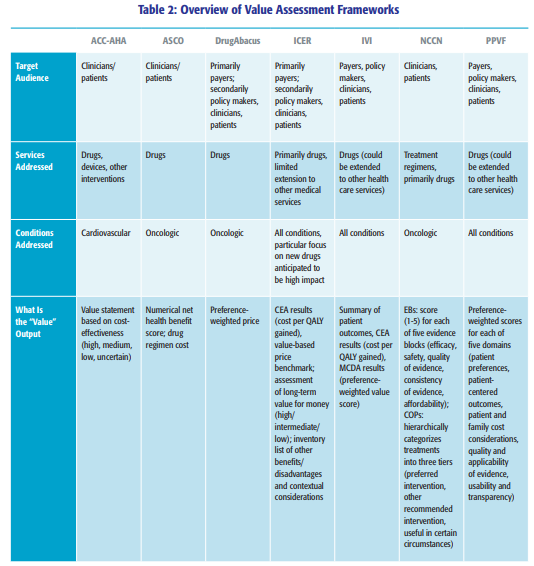

 This year I’ll do the same, among a wonderful team of speakers all touching on aspects of the theme of humanizing health care walking Dr. Osler’s talk. They include:
This year I’ll do the same, among a wonderful team of speakers all touching on aspects of the theme of humanizing health care walking Dr. Osler’s talk. They include: My own talk will address my new friend “TiSH,” an acronym that stands for “Trust, Stress and Health Literacy.” I’ll discuss these three elements as part of a toxic cocktail that prevents people from achieving optimal health. TiSH not only erodes an individual’s health status, but prevents the health system from reaching that elusive Holy Grail, the Quadruple Aim.
My own talk will address my new friend “TiSH,” an acronym that stands for “Trust, Stress and Health Literacy.” I’ll discuss these three elements as part of a toxic cocktail that prevents people from achieving optimal health. TiSH not only erodes an individual’s health status, but prevents the health system from reaching that elusive Holy Grail, the Quadruple Aim.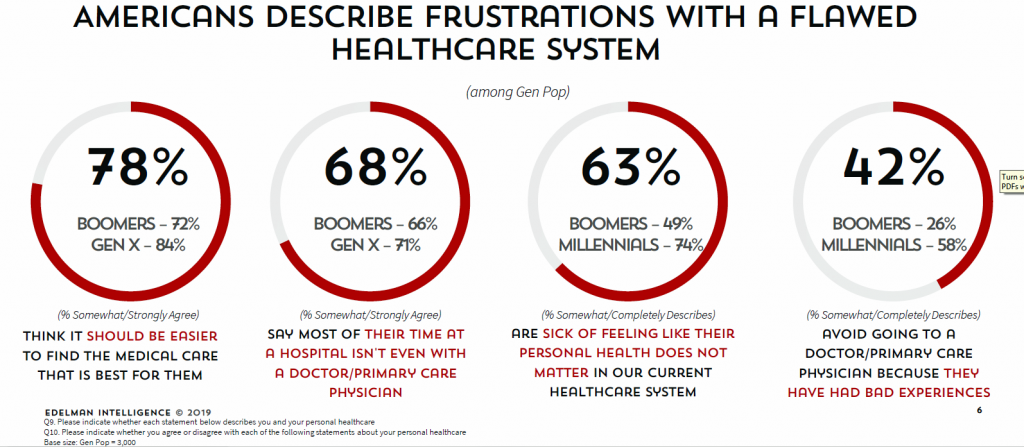
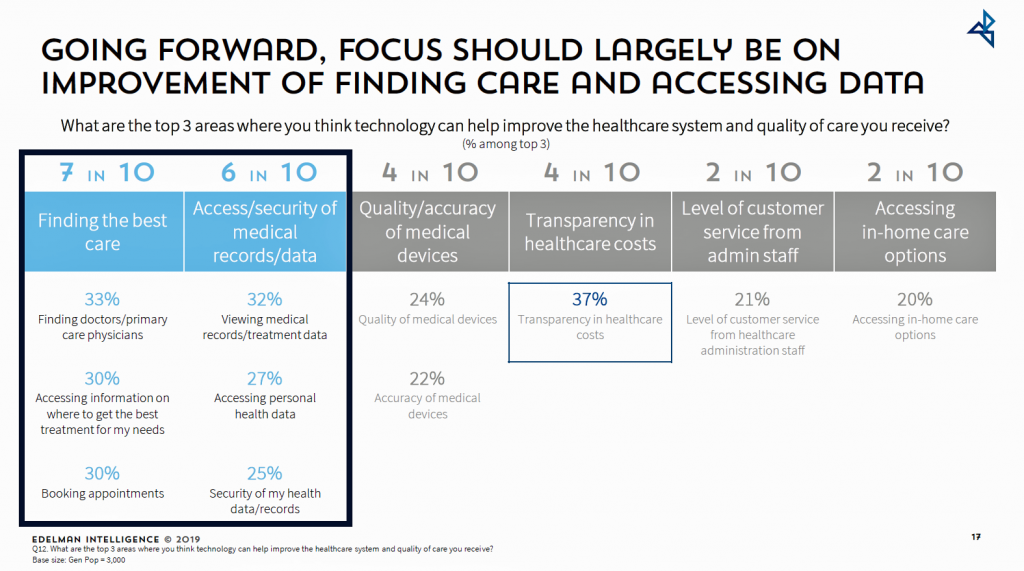 Looking at the future, U.S. consumers identified their top three areas where they think technology can help improve the healthcare system and quality of care received; these were:
Looking at the future, U.S. consumers identified their top three areas where they think technology can help improve the healthcare system and quality of care received; these were: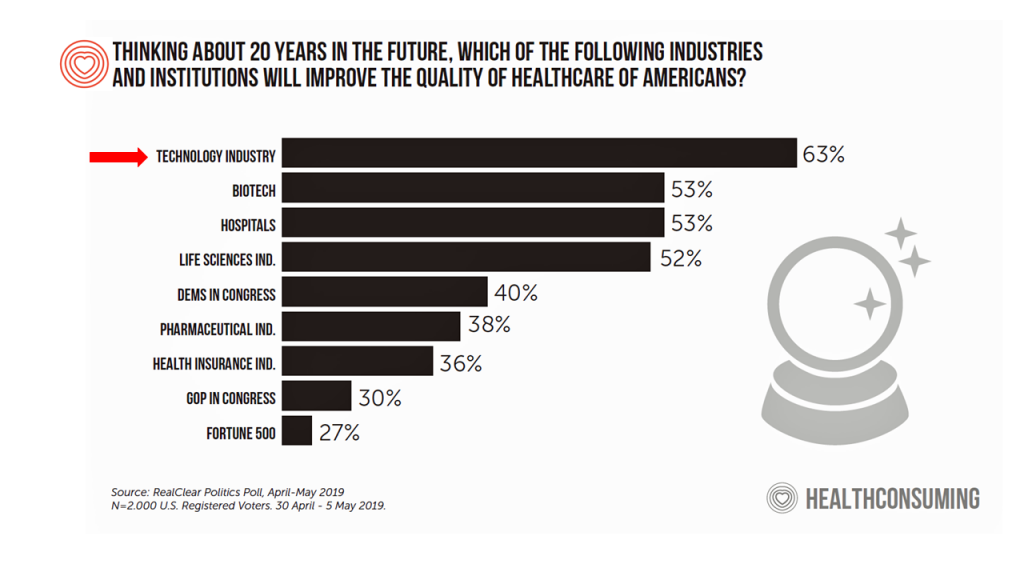 Health Populi’s Hot Points: This week at the Connected Health Conference in Boston, Dr. Joe Kvedar has convened innovators and users of technologies that “connect” patients and clinicians that support the continuum of health care, from prevention and wellness through to remote health monitoring for complex conditions that could once only be tracked and treated from a hospital bed.
Health Populi’s Hot Points: This week at the Connected Health Conference in Boston, Dr. Joe Kvedar has convened innovators and users of technologies that “connect” patients and clinicians that support the continuum of health care, from prevention and wellness through to remote health monitoring for complex conditions that could once only be tracked and treated from a hospital bed. Yes, technology will absolutely underpin improvements, streamlining, enchantment, when those tools are well-designed with the users (patients, clinicians, administrative and financial managers) baked into their focus and workflows.
Yes, technology will absolutely underpin improvements, streamlining, enchantment, when those tools are well-designed with the users (patients, clinicians, administrative and financial managers) baked into their focus and workflows.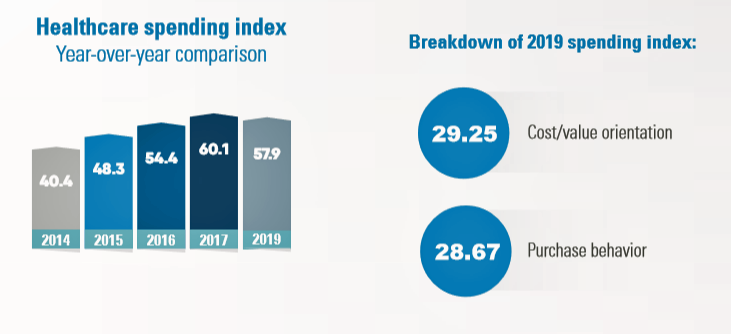 In the U.S., the theory of and rationale behind consumer-directed health has been that if you give a patient more financial skin-in-the-game — that is, to compel people to spend more out-of-pocket on health care — you will motivate that patient to don the hat of a consumer — to mindfully research, shop around, and purchase health care in a rational way, benefit from lower-cost and high-quality healthcare services.
In the U.S., the theory of and rationale behind consumer-directed health has been that if you give a patient more financial skin-in-the-game — that is, to compel people to spend more out-of-pocket on health care — you will motivate that patient to don the hat of a consumer — to mindfully research, shop around, and purchase health care in a rational way, benefit from lower-cost and high-quality healthcare services.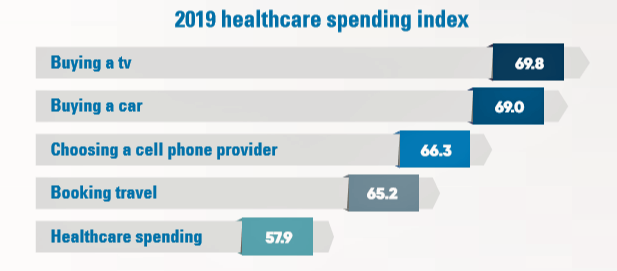 That’s health literacy — more specifically, health insurance literacy — and even after several years of growing adoption of high-deductible health plans, premiums and copayments required from patients, one in two consumers still can’t correctly define the terms of health plan financial engagement.
That’s health literacy — more specifically, health insurance literacy — and even after several years of growing adoption of high-deductible health plans, premiums and copayments required from patients, one in two consumers still can’t correctly define the terms of health plan financial engagement.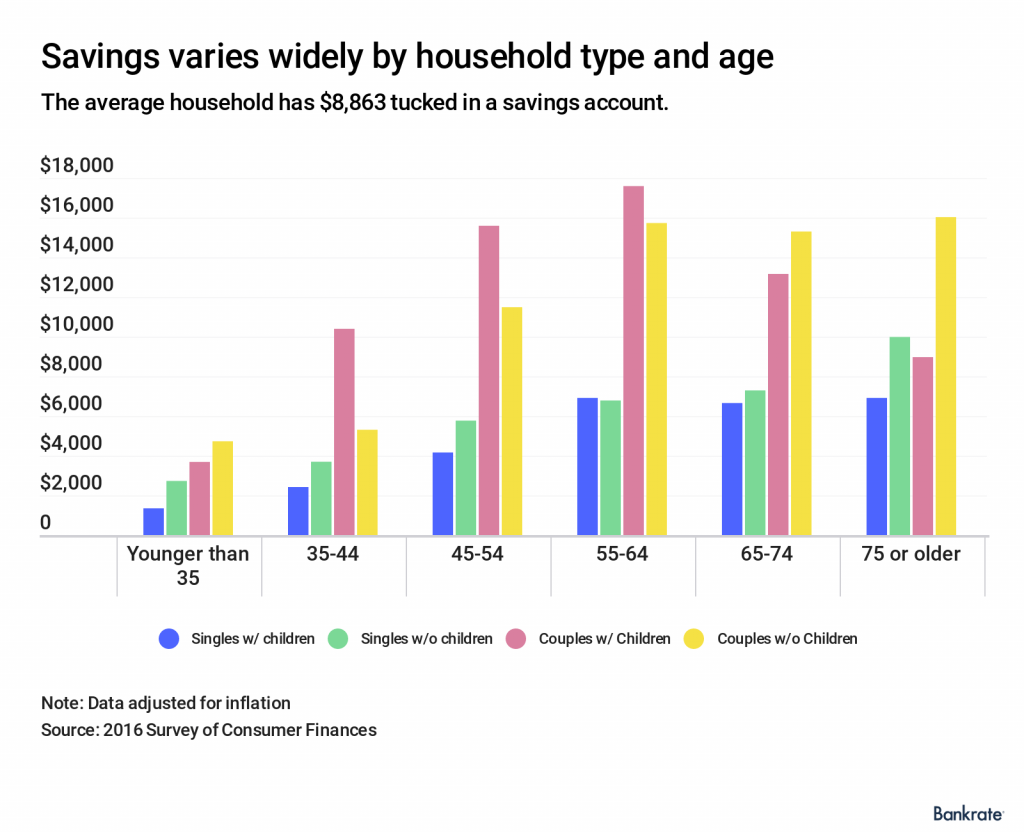 Health Populi’s Hot Points: Another key aspect of health care consumerism when dealing with a high-deductible health plan is saving. Alegeus found that people are making progress in saving more for healthcare — up 13% between 2018 and 2019, which is a significant rise relative to other savings categories in U.S. households.
Health Populi’s Hot Points: Another key aspect of health care consumerism when dealing with a high-deductible health plan is saving. Alegeus found that people are making progress in saving more for healthcare — up 13% between 2018 and 2019, which is a significant rise relative to other savings categories in U.S. households. RSS Feed
RSS Feed
